This syndrome is characterized by the partial or complete absence of one of the X chromosomes in females. This results in a reduction of the total number of chromosomes to 45 (karyotype – 45, X). Thus, this syndrome is also called Monosomy X. Its first description as a syndrome was by Henry Turner in 1938. Later, in 1954, the absence of barr body (inactivated X-chromosome seen in buccal cells) and presence of only one X chromosome was noted. As we saw in Down syndrome, monosomy of X is not the only cause of this syndrome. Mosaicism, deletions and isochromosome have also been shown to cause this condition.
It is well known that, of the two X chromosomes in females, one is inactivated throughout her lifetime. If normal females have only one active X chromosome, then why should the loss of one X chromosome cause abnormal phenotype? The answer lies in the fact that although we speak of inactivated X chromosome, not all genes on that chromosome are being inactivated. There is a small subset of genes on the X chromosomes that are required to be expressed by both chromosomes for normal female development. Thus, individuals who lack one X chromosome fail to develop normal female character.
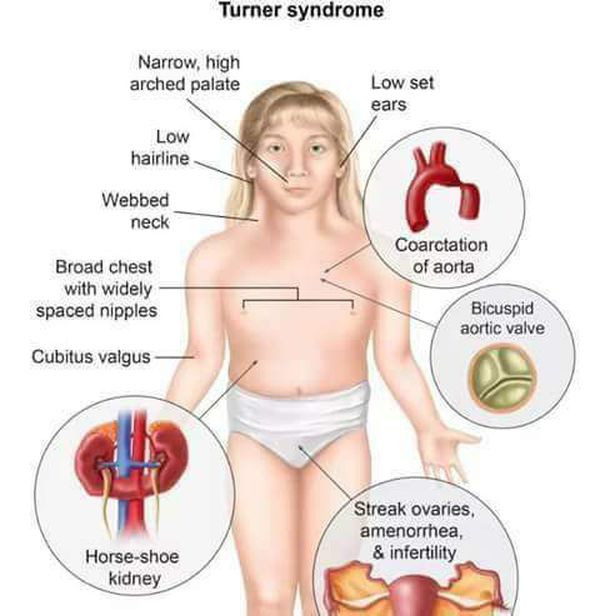
Some of the commonly seen manifestations of Turner syndrome are:
- Primary hypogonadism – poor ovary development
- Short stature
- Minimal breast development
- Broad shield-like chest with widely spaced nipples
- Absence of menstrual periods
- Absence of secondary sexual characteristics
- Horseshoe-shaped kidney
- Inability to produce gametes – sterility
When is Turner syndrome diagnosed?
Healthcare providers may diagnose Turner syndrome at any stage of a child’s development. Sometimes, the condition gets spotted before birth:
- Maternal serum screening is a blood draw from the mother. It checks for signs showing an increased chance of a chromosomal problem with the baby. This screening is more common in women who are pregnant at an older age.
- Amniocentesis and chorionic villous sampling check the amniotic fluid or tissue from the placenta. Healthcare providers perform a karyotype analysis on the fluid or tissue. The results could show that the baby has Turner syndrome.
- Ultrasound during pregnancy may show that the baby has some features of TS. The healthcare provider may see heart problems or fluid around the neck.
Other times, children receive a diagnosis soon after birth or during early childhood because of their symptoms. But some people aren’t diagnosed with Turner syndrome until they reach adulthood. These women may go through puberty and get their periods. But they often have early ovarian failure (early menopause).
How is Turner syndrome treated?
Besides care for related medical problems, Turner syndrome (TS) treatment often focuses on hormones. Treatments may include:
- Human growth hormone: Injections of human growth hormone can increase height. If treatment starts early enough, these shots can increase the final height of people with TS by several inches.
- Estrogen therapy: Often, people with TS need estrogen, a female hormone. This type of hormone replacement therapy can help girls develop breasts and begin menstruation. It can also help their uterus grow to a typical size. Estrogen replacement improves brain development, heart function, liver function and skeletal health, too.
- Cyclic progestins: These hormones are often added at age 11 or 12 if blood tests note deficiency. Progestins will induce cyclic menstrual periods. Treatment is often started with very low dosages and then gradually increased to simulate normal puberty.