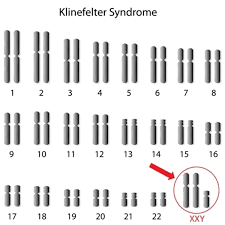
The presence of an additional X chromosome in males causes abnormal sexual development and is described as Klinefelter syndrome. This set of characteristics was first described by Harry Klinefelter in 1942. In 1959 it was shown to be due to the presence of an additional X chromosome in males by the presence of barr bodies in these males (normal males do not show barr body). The additional X chromosome results in an increase in the total number of chromosomes to 47 (karyotype 47, XXY). It has an overall incidence of 1 in 1000 live male births. While most patients show the XXY condition, individuals showing variations like XXXY or XXYY have also been reported.
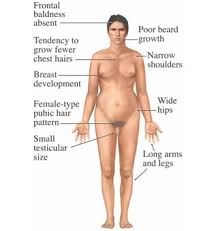
The additional X chromosome arises due to non-disjunction during meiosis. Due to this, the gamete contains two X chromosomes rather than one. When such an egg containing XX is fertilized by sperm containing Y, an XXY zygote is formed that develops into a Klinefelter male. The extra X chromosome may be either of maternal or paternal origin, but it is more often to be of maternal origin. Individuals with this syndrome show hypogonadism and reduced fertility. These males do no develop masculine secondary sexual characteristics and show female type characteristics. Some of the clinical manifestations include:
• Primary male hypogonadism
• Reduced facial, body and pubic hair
• Small and soft testes
• Slight learning difficulties
• Increased breast tissue – gynacomastia
• Long limb bones and lanky body
• Azoospermia – absence of sperm production leading to infertility
Causes of Klinefelter syndrome
Klinefelter syndrome is caused by an additional X chromosome. This chromosome carries extra copies of genes, which interfere with the development of the testicles and mean they produce less testosterone (male sex hormone) than usual. The extra genetic information may either be carried in every cell in the body or it may only affect some cells (known as mosaic Klinefelter syndrome). Klinefelter syndrome is not directly inherited – the additional X chromosome occurs as a result of either the mother’s egg or the father’s sperm having the extra X chromosome (an equal chance of this happening in either), so after conception the chromosome pattern is XXY rather than XY. This change in the egg or sperm seems to happen randomly. If you have a son with the condition, the chances of this happening again are very small. But the risk of a woman having a son with Klinefelter syndrome may be slightly higher if the mother is over 35 years of age.
Testing for Klinefelter syndrome
Klinefelter syndrome is not necessarily anything serious, but treatment can help reduce some of the symptoms if necessary. In many cases, it’s only detected if a man with the condition undergoes fertility tests. Suspect Klinefelter syndrome after a physical examination and may suggest sending off a sample of blood to check reproductive hormone levels. The diagnosis can be confirmed by checking a sample of blood for the presence of the extra X chromosome.
Treatments for Klinefelter syndrome
There’s no cure for Klinefelter syndrome, but some of the problems associated with the condition can be treated if necessary.
Possible treatments include:
- testosterone replacement therapy
- speech and language therapy during childhood to help with speech development
- educational and behavioural support at school to help with any learning difficulties or behaviour problems
- occupational therapy to help with any co-ordination problems associated with dyspraxia
- physiotherapy to help build muscle and increase strength
- psychological support for any mental health issues
- fertility treatment – options include artificial insemination using donor sperm or possibly intracytoplasmic sperm injection (ICSI), where sperm removed during a small operation are used to fertilise an egg in a laboratory
- breast reduction surgery to remove excess breast tissue