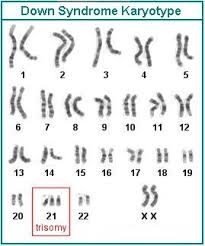
Down syndrome was one of the first reported chromosomal abnormalities in humans. It was described as Mongolian Idiocy by John Langdon Down in 1866. It wasn’t until 1959 that it was shown to be caused by the presence of an extra chromosome 21, resulting in an increase of number of chromosomes to 47 (karyotype 47, XX / XY, +21). Thus, this disorder is also known as trisomy 21 or Down syndrome. With an incidence of 1 in 800 live births, this is one of the common trisomies seen in humans. This incidence increases to 1 in 350 when the woman conceives beyond 35 years of age and to 1 in 25 when she conceives beyond 45 years. Down syndrome is caused by trisomy 21 in almost 90% of the cases. 6% of the cases are also shown to be caused by a translocation rather than a numerical change and the other 4 % are known to be caused by mosaicism
There are many phenotypic manifestations that are typical in patients of this syndrome. However, as in other syndromes, not all affected individuals show all the symptoms. Any single individual usually expresses only a subset of the manifestations. Some of the most common are:
- Flat face, round head, and typical epicanthic fold of the eyes
- Short, broad hands
- Mental retardation
- Hypotonia – poor muscle tone
- Short stature
- Protruding furrowed tongue
- Mild to moderate developmental disabilities
- Typical dermatoglyphic patterns (palm and fingerprint patterns)

The most common cause of this trisomy is the non-disjunction or the failure of separation of the chromosomes during meiotic division. Due to this one of the gametes undergoing fertilization contains two copies of chromosome 21 instead of the normal one copy (gametes are haploid containing one copy of each chromosome). This non-disjunction can occur at either meiosis I or II. Chromosomal analysis has shown that 75% of the cases are due to nondisjunction occurring at meiosis I. When such a gamete is fertilized by a normal gamete, it results in trisomy 21.