- 1.2 Concept of Nutrition
- 1.3Concept of Nutrition and Health
- l.4 Concept of Nutrition and Cultural Practices
- 1.5 Concept of Nutrition and Food Habits
- 1.6 Concept of Balanced Diet
1.2 CONCEPT OF NUTRITION
There are some concepts in nutrition which we need to understand.
Nutrition: Nutrition is a physiological fact which helps organisms to assimilate the nutrients of the food for proper maintenance and growth and development of the body.
Optimum nutrition: When a person receives and utilises essential nutrients in proper proportions according to the requirements of the body it is called optimum nutrition.
Nutritional status: It is the condition of the body which relates to consumption and utilisation of food. The nutritional status of a person may be either good or bad.
Good nutritional status: It is the state of a well-balanced diet in which all the essential nutrients is supplied to meet the body’s requirements. Such a person is characterized with optimum nutrition.
Poor nutritional status: It refers to the state of inadequate or excessive intake or improper utilisation of the nutrients to meet the body’s requirements, Thus, overeating is also considered as poor nutritional status and this may result into overweight person.
Malnutrition: It refers to the effects on the human body due to excess or inadequate dietary intake. A person with poor nutritional status is most likely to be malnourished.
Under-nutrition: It refers to the state of low food intake in human body
1.3 CONCEPT OF NUTRITION AND HEALTH
According to Ministry of Women and Child Development (2006):
“Nutrition is the science of food and its relationship to health.
Good Nutrition is a fundamental requirement for positive health, functional efficiency and productivity.
Nutritional status is internationally recognized as an indicator of national development.
Nutrition is both an input into and an output of the development process.
A well nourished healthy workforce is a pre-condition for successful economic and social development, and as such food security, nutrition, health and sanitation are the responsibility of all development sectors and indeed of all citizens.
In many developing countries including India, economic productivity has increased and impressive efforts have been made in nutrition interventions, but significant improvement in nutritional status has not accompanied these advances.
Investing in nutrition has both economic and social benefits.
Improved nutritional status has an enhancing effect on investments in other sectors such as health, education and agriculture. Moreover, the enormous social and financial costs of malnutrition are averted when nutritional status is improved.
Nutrition and health are inseparably related. Good health implie good nutrition. Nutrition is increasingly being recognized as an important indicator of development at national as well as international levels. Nutritional well being of a population is considered as an economic asset and a pre-requisite for .national development.
The signs of good nutritional status are shiny hair, smooth skin, clear eyes and alert expression and firm flesh. A well developed physical feature reflects good nutritional status of a person. A person should have correct weight in relation to his/her height. His/her physical and mental responses should be normal. Good nutritional status of a person is also reflected by his/her energy and resistance to combat diseases. Good nutrition helps a person have regular leep and elimination habits. It may increase a person’s life span. A person with a good nutritional status can enjoy life fully.
The signs of poor nutritional status are characterized with poor physique, very little stamina, dull hair, dull eyes, slumped posture and depression. He/she may be grossly overweight or underweight. The three important aspects namely the diet, sleep and elimination habits may be irregular for a poor nutritional status person.
There has been a conquest over nutritional deficiencies in India – Florid Nutritional Deficiency Syndromes like Pellagra, Beri Beri, Scurvy, Kwashiorkar have disappeared, famines are no more, severe malnutrition among preschoolers has been reduced appreciably and nutritional status of adults has improved significantly. But still the high levels of malnutrition continue to influence morbidity and mortality rates in the country.
The challenges that still remains includes:
- High malnutrition levels particularly in women and children,
- Undernutrition,
- Micronutrient malnutrition,
- Emerging diet related diseases,
- High mortality rates-infant mortality rate, under-five mortality rate and maternal mortality ratio,
- Inadequate access to health care facilities, and
- Poor immunization coverage.
1.4 CONCEPT OF NUTRITION AND CULTURAL PRACTICES
Social and Cultural Factors ill Nutrition
Social factors and cultural practices in most of the countries have an impact on what people prefer to eat. in many countries practices are specifically designed to protect and support good health; providing women with rich, energy dense foods during the first months following childbirth. It is, however, true that some traditional food practices and taboos in some societies may contribute to nutritional deficiencies among some particular groups of the population.
Traditional food practices may not always be a scientific one leading to balanced diet; and cultural taboos related with some essential food items in some societies can lead to malnutrition because of nutritional deficiencies.
Nutrition: Parental Choice
Children and adolescents all over the world share food preferences with their parents rather than their friends in general. Since birth, parents use to make most food choices for their children, which may be influenced by the foods that are available in their surroundings. Although there is variability within a culture, most parents have some common choice about food.
Why children and adolescents all over the world share food preferences with their parents rather than their friends? In human beings, intake of food is culturally conditioned rather than being wholly biological or natural. A human baby grows up in a family learning to speak, gets acquainted with do’s and don’ts as per custom. In the same way the baby also gets accustomed with ‘what to eat and what not’ as per norms of the family and dictated by the parents. After initial cultural patterning, a baby comes out of the family and mixes with friends, who are also conditioned, culturally, by their respective families. Perhaps, that is the rea on that children share their food preferences with their parents, and not with their friends.
Unusual feeding practices of the newborn
It has been noticed in most of the countries that there exist differences in feeding practices of the newboms at birth if they are delivered at a medical centre or at home. Aboud (2002) is of the opinion that before giving breast milk, Ethiopian newboms might be given a spoonful of soft rancid butter or warm water with sugar to oil the pipes and sweeten the vocal cords..
Unfortunately, many new urban mothers have the misguided belief that they do not have enough milk and their baby needs more nutrients to grow. Consequently, they regularly supplement breastfeeding with other foods and liquids such as cereal, fruit, cow’s milk, and tea in the first few months; the supplements in turn impair mother’s milkflow.It should be remembered thatbreast milkbyitselfprovides everything infants need. The number of mothers giving only breast milk in the first 3 months varies from 9percentinTurkey to50per centinIndia and 84percentinEthiopia.
WeanIng food practices
Some of the societies prefer to introduce solid food early to their babies for weaning, while other prefers the reverse. In Africa and Asia many mothers believe that one can wait until children have teeth at one year before feeding them solid food. Others believe that a special kind of traditional food with lots of mass but few calories will atisfy children’s hunger. Both of these diets lead to malnutrition.
In most of the countries the most common foods missing from children’s diets are fruits arid vegetables, and in some cases, milk. Even in warm tropical climates where fruits and vegetables are plentiful, there is the belief that fruits and vegetables give children diarrhea. Ofcourse, loose stools for one day are not the same as watery stools for three days straight. Furthermore, once breastfeeding ceases, children in rural developing areas rarely drink cows’ milk (Aboud, 2002).
1.5 CONCEPT OF NUTRITION AND FOOD HABITS
Nutrients and healthy life
Nutrients, which we obtain through food, have vital effects on physical growth and development, maintenance of normal body function, physical activity and health. Nutritious food is, thus needed to sustain life and activity. Our diet should provide all essential nutrients in required amounts.
Man needs a wide range of nutrients to lead a healthy and active life and these are derived through the diet he consumes daily. The components of his diets must be chosen judiciously to provide all the nutrients he needs in adequate amounts and in proper proportions (ICMR, 2004). In many countries though cheap and nutritious foodstuffs are readily available, it is noticed that millions of children are chronically malnourished and every year many ofthem die from mild to moderate malnutrition.
Breastfeeding and complementary feeding
If brea tfeeding (including exclusive breastfeeding for the first six months and continued breastfeeding for the next six months) is universalized it will serve as the single most effective preventive intervention. Exclusive breastfeeding for the first ix months can cut down about 15 per cent of all child deaths. However, in India only about 20 per cent women are able to practice exclusive breastfeeding for six months. Adequate complementary feeding between six months to 24 months could prevent an additional 6 per cent of all such deaths. This means that extending coverage of exclusive breastfeeding and complementary feeding could save over 450,000 child deaths each year in India (Ministry of Women and Child Development 2006, Government of India).
Thus, breast feeding is essential for first six months of life to the babies because it save their life as single most effective means to protect the child from many diseases, and thereby decreasing child mortality .
Food habits and their origins
All people have their liking, disliking and beliefs about food. Many people are conservative in their food habits. They tend to like what their mothers cooked forthem when they were young, the foods that are served on festive occasions and those eaten with friends. Traditional customs, however, always play an important role in food habits.
What one society regard a normal or even highly desirable, another society may consider revolting or totally inedible. Animal milk is commonly consumed and liked , in most parts of Asia, Africa, Europe and the America , but in China it is rarely taken. Foods like lobsters, crabs and shrimps are con idered delicious by many people in Eur pe and North America, but are revolting to many people in Africa and Asia, especially tho e who live far from the sea. The French eat hor e meat, whereas the English generally do not. Many people will delightedly consume the flesh of monkeys, snakes, dogs and rats or will eat certain insects, however, many others find these foods most unappealing. Religion may have an important role in forbidding the consumption of certain foods. For example, Muslim and Jewish do not consume pork, and Hindus do not eat beef.
Food Habits: The Changing Scenario
It is often stated that fo d habits in a society seldom or never change and are difficult to change. This is 110ttrue; in many countries the current staple foods are not the same as those eaten even a century ago. Food habits do change, and are influenced by the changing life styles.
Food preferences are not made and abolished by whims and fancies. More often, the adjustments are generated by social and economic changes that take place throughout the community or society. The issue is often not what food are eaten but rather how much of each food is eaten and how the consumption is distributed within the society or within the family,
The tendency of many wage-earners to spend almost all their wages within a few days of receiving them often results in a family diet of varying nutritive value. The family eats much just after one payday than just before the next. Wages arc often paid monthly, and there seems little doubt that a change to weekly payment of wages would improve the diet of wage-earners and their families. In general, when mothers, rather than fathers, have some control over finances, the family diet is likely to be better,
Nutritional advantages of traditional food habits
Food habits in most of the traditi naJ ocieties in developing countries arc good ill general. Eating protein-rich foods such as insects, snakes, baboons, mongooses, dogs, cats, unusual sea foods and snails is definitely beneficial. Some African tribes puncture the vein of a cow, draw, off a calabash of blood, an-est the bleeding and consume the blood, usually after mixing it with milk. Blood is a rich food, and mixed with milk it is highly nutritious.
In some pastoral societies drinking of soured or curdled milk is in practice rather than fresh. The souring of milk has little effect on its nutritive value but often sub. tantially reduces the number of pathogenic organisms present in body. Communities where milking is not hygienically performed the milk is likely to be contaminated, it is safer to drink our rather than fresh milk. Boiled milk is still safer.
Many societies, for example in Indonesia and in parts of Africa, partly ferment foods before con umption, Fermentation may both improve the nutritional quality and reduce bacterial contamination of the food.
Advantage of the traditional foods is that they are highly nutritious.
Food taboos: A taboo reiat d to food may be followed by a nation, by a tribe or by certain groups in the society.Within the society, different food customs maybe practiced by women or children or by pregnant women or female children. Sometimes traditional food customs are practiced by a particular age group, and in other instances a taboo may be linked with an occupation such as hunting. A taboo may also be imposed because of some particular event such as an illness or . an initiation ceremony.
Many taboos concern the consumption of protein-rich animal foods, often by those groups of the community most in need of protein. A common taboo in Africa against the consumption of eggs is rapidly disappearing. This taboo usually applies to females, who are said to become sterile if they eat eggs. Some societies forbid some foods to women during pregnancy that hamper their balanced diet.
Reasons behind food taboos in many countries are mainly due to prevailing food customs which are often governed by their religious practice.
Harmful new habits: All new food habits are not good for nutrition. Locally available complementary foods as well as home-produced and traditionally fed, are often as or more nutritious than the manufactured baby foods.
Another particularly misleading type of advertising relates to the glucose products said to provide “instant energy”. Energy is present in large amounts in nearly all the cheaper foods. Similarly, drinks advertised as “rich in vitamin C” are usually unnecessary, since few children suffer from vitamin C deficiency. Vitamin C can be obtained just as well from fruits such as guavas, mangoes and citrus, or from a range of vegetables.
In some countries the staple food has remained unaltered, but the form in which it is preferred may have changed over the years. In many part of the world highly milled cereals have replaced traditionally lightly milled and more nutritious wheat, rice and maize. In the United Kingdom and the Russian Federation, white bread has been replaced by brown or whole-grain breads, and in East Africa highly milled maize meal is often purchased and has replaced lightly milled maize flour. Urbanization, modernization and sophistication have often led to diets in which a greater percentage of energy intakes come from sugar and fats, and to increased consumption of salt. All of these are generally undesirable changes from a nutritional standpoint.
We think the reasons behind harmful new food habits in most of the countries are: (i) disregard for own cultural tradition, (ii) imitation of so-called ‘western culture’ in the name of ‘globalization’ and (iii) a false sense of modernization.
1.6 CONCEPT OF BALANCED DIET
What is balanced diet?
Our body requires a continuous supply of nutrients, These nutrients are utilized by the body in order to maintain health. The nutrients ought to be supplied daily in the right proportion for optimum utilisation and proper body maintenance. This can be achieved by taking a balanced diet every day (Joshi, 1992).
Dietary habits of population in different countries of the world have been determined mainly by the local availability of food and local practices. For maintaining good health and active life, diets should be planned in .proper way.
The nutritional requirements of an individual and the dietary allowances for a group or a population are distinctly different. It depends upon the age, body weight and the physiological and metabolic status of the individual. Side by side, individual variation within the group, quality of diet, effect of cooking and processing, and bioavailability of nutrient should also be taken into consideration.
The quantities of food’ needed to meet the nutrient requirements vary with age, gender, physiological status and physi al activity. A balanced diet should provide around 50-60 per cent of total calories from carbohydrates, 10-15 per cent from proteins and 20-30 per cent from visible and invisible fat (JCMR, 2010). In addition, a balanced diet should provide other non-nutrient such a dietary fibre, antioxidants and phytochemical. which give positive health b nefits, Antioxidant such as vitamins C and E, beta-carotene, riboflavin and selenium protect the human body from free radical damage. Other phytochemicals uch a polyphenols, fiavones, etc., also afford protection again t oxidant damage. Spices like turmeric, ginger, garlic, cumin and c10 es arc rich in antioxidants.
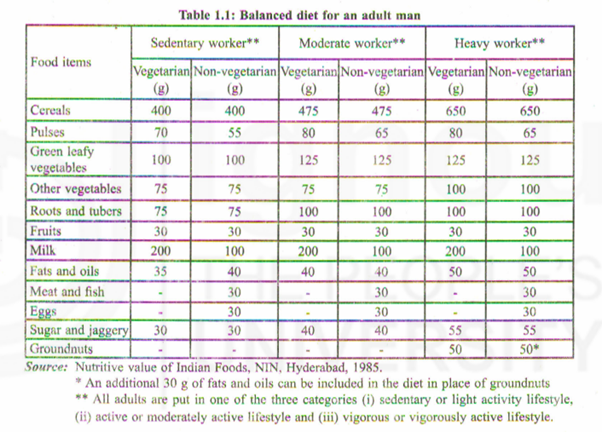
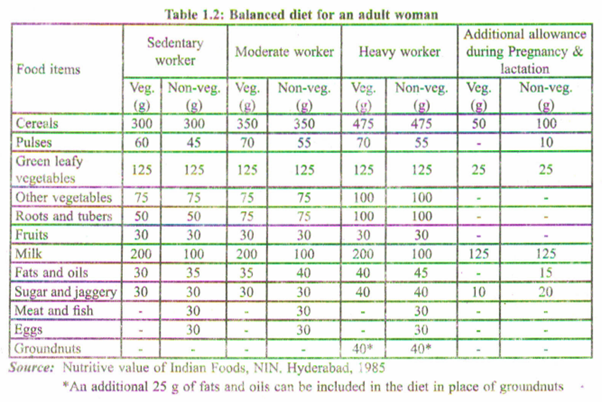
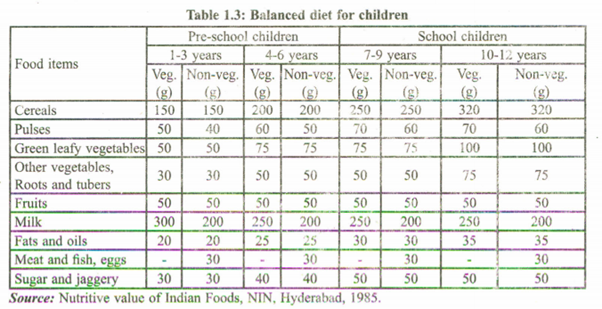
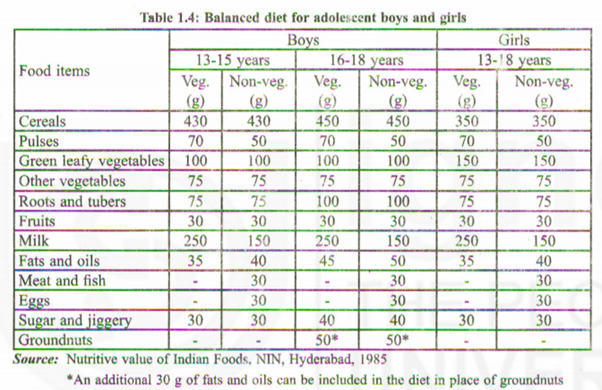
A diet which contains adequate amounts of necessary nutrients required for healthy growth and activity is called balanced diet. The recommended food and dietary allowances as per the ICMR (1981, 2010) have been shown in Tables 1.4. These furnish the food items that are required to be eaten in a balanced diet by the different age groups.
Dietary Standards – What are they?
Dietary standards, regardless of the name they go by-Recommended Dietary Allowances, Recommended Nutrient Intakes, Recommended Daily Amounts of Nutrients, or Safe Intake’s of Nutrients – are the average daily amounts of essential nutrients estimated to be sufficient to meet the physiological needs of practically all healthy persons in a group with specified characteristics.
Some internationally used tenninologies can be mentioned. In 2007, United Nations University (UNU) in collaboration with World Health Organization (WHO), Food and Agriculture Organization (FAO) and others convened a group to harmonise nutrient-based dietary standards. They decided that the term Nutrient Intake Values (NIV) should include, Average Nutrient Requirement (ANR) and Upper Nutrient Limit (UNL).
If dietary intake covers about 98 per cent of the population referring to Recommended Dietary Allowances, then it may be taken as dietary standard.
Nutrition requirement and recommended dietary allowances (RDA)
Recommended Dietary Allowance (RDA): The average daily dietary nutrient intake level which is sufficient to meet the nutrient requirement of nearly all (more precisely about 97.5%) healthy individuals in a particular life stage and gender group i called recommended dietary allowance or RDA.
Adequate Intake: A recommended average daily intake level based on observed or experimentally determined approximations or estimates of nutrient intake by a group (or groups) of apparently healthy people, that are assumed to be adequate used when an RnA cannot be determined. In Indian context, this is referred to as Acceptable Intake.
Tolerable Upper Intake Level (UL): The highest average daily nutrient intake level that is likely to pose no risk to health condition for almost all the individuals in a general population is called Tolerable Upper Intake Level.
Estimated Average Requirement (EAR): The average daily nutrient intake level i estimated to meet the requirement of half of the healthy individuals in a particular life stage and gender is called Estimated Average Requirement. It means that the needs of the other half of the population will not be met by this amount. The RnA is derived from (i) the individual variability, and CH) the nutrient bioavailability from the habitual diet.
Individual variability: Definition ofRDA takes into account the variability that exists in the requirement of a given nutrient between individuals in a given population group. The distribution of nutrient requirement in a population group is considered normal.
Bio-availability: Bio-availabillty of a given nutrient from a diet is, the release of the nutrient from the food and its absorption in the intestine. It is the level of the nutrient that should be present in the diet to meet the nutritional requirement. This bio-availability factor is quite important in case of calcium and protein and trace elements like iron and zinc. In case of iron, the amount to be present in the diet is 20-30 times higher than the actual iron requirement to account for the low bioavailability of iron from a given diet, particularly a cereal-based diet.
In India, the first attempt to define nutrient requirements and desirable dietary intakes of nutrients for Indians to maintain good health was made by the Nutrition Advisory Committee of the Indian Research Fund Association [Now Indian Council of Medical Research (ICMR)] in 1944. This followed the recommendations made by the Technical Committee of the Health Committee, League of Nations in 1936, Food and Nutrition Board of the National Research Council, USA, 1944 and Report of the Committee of Nutrition, British Medical Association 1933. At that time, requirement and allowances of only energy, protein, iron, calcium, vitamin A, thiamine, riboflavin, ascorbic acid and vitamin D for Indians were considered.
Considering these recommendations of nutrients, a typical balanced diet based on habitual Indian dietary habits was formulated to provide all the nutrients for a normal adult man of 55 kg and a normal adult woman of 45 kg body weight. This was used to demonstrate that the diet then consumed by Indians, particularly by the poor, was deficient in several nutrients and could be improved by inclusion of some protective foods. Now we consider 60 kg for adult males and 50 kg for adult females.
However, in practice, fluctuations in intake may occur depending on the food availability and demands of the body. But, the average requirements need to be satisfied over a period of time. The diet that one consumes must provide adequate calories, proteins and micronutrients to achieve maximum growth potential. There may be situations where adequate amounts of nutrients may not be available through diet alone. In such high risk situations where specific nutrients are lacking, foods ‘.fortified with the limiting nutrient(s), such as iodized salt, double fortified salt with iron and iodine are necessary.
Why additional diet is required during pregnancy and lactation?
In India, it is observed that diets of women from the low socioeconomic groups are essentially similar during pre-pregnant, pregnant and lactating periods. Consequently,
there is widespread maternal malnutrition leading to high prevalence of low birth weight infants and very high maternal mortality. Additional foods are required to improve pregnancy weight gain and birth weight of infants. Pre-pregnant Body Mass Index (BMI), maternal age and rate of pregnancy weight gain must be considered in monitoring the calorie recommendation to the pregnant women.
What are the nutrients that require special attention?
The daily diet of a woman should contain an additional 350 K. calories and 0.5 g, 6.9 g and 22.7 g of protein during first, second and third trimester of pregnancy, respectively. Some extra amounts of micronutrients are also required during these physiological periods. Folic acid, taken throughout the pregnancy, reduces the risk of congenital malformations and increases the birth weight. The mother as well as the growing foetus needs iron to meet the high demands of erythropoiesis (RBC formation). Calcium is essential, both during pregnancy and lactation, for proper formation of bones and teeth of the offspring, for secretion of breast-milk rich in calcium and to prevent osteoporosis of mother. Similarly, iodine intake ensures proper mental health of the growing foetus and infant. Vitamin A is required during lactation to improve child survival. Besides these, nutrients like vitamins Band C need to be taken by the lactating mother.
How can the pregnant and lactating women meet nutritional demands?
The pregnant/lactating woman should eat a wide variety of foods to make sure that her own nutritional needs as well as those of her growing foetus are met. There is no particular need to modify the usual dietary pattern. However, a proper combination of cereals, pulses and nuts also provides adequate proteins.
Mineral and vitamin requirements are met by consuming a variety of seasonal vegetables particularly green leafy vegetables, milk and fresh fruits. Bioavailability of iron can be improved by using fermented and sprouted grams and foods rich in vitamin C such as citrus fruits. Milk is the best source of biologically available calcium. Though it is possible to meet the requirements for most of the nutrients through a balanced diet, pregnant/lactating women are advised to take daily supplements of iron, folic acid, vitamin B and calcium.
Why do children and adolescents require morefood?
Childhood and adolescence are periods of continuous growth and development. An infant grows rapidly, doubling its birth weight by 5 months and tripling it by Iyear of age. During the second year, the child increases not only in height by 7-8 cm but also gains 4 times of its birth weight. During the pre-adolescent period the child grows, on an average, 6-7 cm in height and 1.5 to 3 kg in weight every year and simultaneously development and maturation of various tissues and organs take place.
Adolescent period (teenage) is spread almost over a decade. It is characterized by rapid .increase in height and weight, hormonal changes, sexual maturation and wide swings in emotion. Adolescent growth spurt starts at about 10-12 years in girls and two years later in boys. The annual peak rates for height and weight are 9-10 cm and 8-10 kg. Development of critical bone mass is essential during this period as this forms the ground for maintaining mineral integrity of the bone in later life. The pattern and proportion of various body components like body water, muscle mass, bone and fat increase during the entire childhood and adolescence to reach adult values by about 18 years of age.
Adolescent girls are at greater physiological stress than boys because of menstruation. Their nutritional needs are of particular importance as they have to prepare for motherhood. Growing children and adolescents particularly require more calcium. Though recommended dietary allowances for calcium are about 600-800 mg/d·only, it is desirable to give higher quantities of calcium for adolescents to achieve high peak bone mass. Young children below the age of 5 years should be given lessbulky foods, rich in energy and protein such as legumes, pulse , nuts, edible oil/ ‘. ghee, sugar, milk and eggs.
Older children and adolescents should consume plenty of milk to fulfill the high calcium requirements. Cooking oils/ghee (25-50g) should be consumed. Over indulgence in fats may be avoided. Excessive salt intake should be avoided particularly by children having a family history of hypertension. Adolescence is the vulnerable stage for developing wrong food habit a well as bad habits like smoking, chewing tobacco or drinking alcohol. These should be avoided. In addition to consumption of a nutritious well balanced diet, appropriate lifestyle practices and involvement in physical activity uch a games/sport should be encouraged among children and adolescents.
Human Nutrient Requirements
In the wake of reports by the Food and Agriculture Organization (FAO) on calorie and protein in 1950 and J 957 respectively, an attempt was made by ICMR in . 1958 through its Nutrition Advisory Committee (NAC) to revise protein and calorie requirement of Indians, based on data available at that time. In 1968, the requirements of all nutrients except energy were reviewed by an Expert Committee constituted by ICMR.
Energy allowances for Indians, which were recommended in 1958, had not been revised till 1988. Tn 1988, an Expert Group was constituted by the ICMR. This Indian Expert Group, while following the new guidelines of the Joint FAO/WHO/ UNU Consultative Group of 1985, also considered the updated data on Indians that had accumulated after 1973, to define the energy and protein requirements of Indian . This Expert Group also defined the r quirement . of other nutrients like fat, vitamin D and vitamin A. This Expert Group included in it recommendations several additional nutrient such a dietary fibre, electrolytes, phosphorus, vitamin E and vitamin K or dietary factors not considered by the earlier TCMR Expert Committees and made provisional recommendations on their desirable intake to maintain good health. Energy allowances for Indians were further revised in 2010 (Table 1.5).
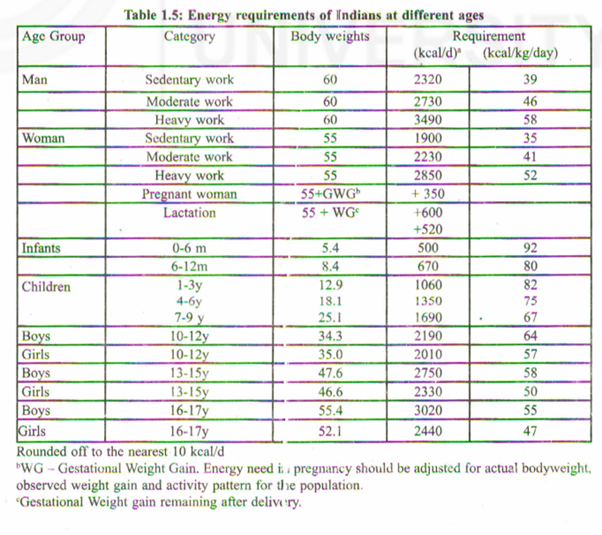
‘Energy needs of children and adolescents have been computed for reference children and adolescents; these reference children were assumed to have a moderate daily physical activity level. The actual requirement in specific population groups should be adjusted for the actual weight and physical activity of that population, especially when computing the gap between energy requirement and actual intake that needs to be filled by supplementation progranimes.
Influencing change for the better
What can health workers or nutritionists in a community do about food habits, old and new? They can:
- protect, support and help preserve many of the excellent existing food habits that are nutritionally valuable;
- respect the knowledge and customs of the people in the community in which they work;
- set good examples in their own households by adopting good food habits;
- influence respected local leaders to state publicly that they themselves have dropped undesirable food taboos, and arrange for them, when occasion arises, to eat “forbidden” foods in public;
- persuade people not to abandon good food habits under the influence of “sophisticates” back from the city who may try to discourage rural dwellers from eating nutritious traditional foods such as locusts or lake flies or to encourage the consumption and production of European-type vegetables in place of better traditional ones;
- explain the disadvantages of highly refined cereal flours if they have become popular in the area, and advocate the consumption of a range of cereals in the local diet;
- take the steps to protect, support and promote breast-feeding and to eliminate all promotion of breast milk substitutes;
- discourage poorer families from purchasing manufactured baby foods, and encourage the use of locally available complementary foods;
- issue informational material to help stop the spread of bottle-feeding and the unnecessary purchase of expensive baby foods;
- strive, through civil service or local authority organizations, for the introduction of the payment of weekly wages instead of monthly wages to employees, and influence labour and trade union leaders to do the same and
- take steps to introduce good feeding practices in the local schools and otherinstitutions.
Purpose of diet surveys
- Diet surveys are carried out to assess what people eat, qualitatively and quantitatively.
- find out whether the .existing dietary patterns are satisfactory or not.
- know the inadequacies in the existing dietary pattern.
- find out the association between diet and disease, e.g.; nutrition deficiency disease.
- formulate plans to improve the existing dietary pattern through final nutrition programmes at the national level.
Nutritional indices in adults
The international standard for assessing body size in adults is the Body Mass Index (BMI). BMI is computed using the formula: ~
BMI = Weight (kgj/Heighf (m’),
We can find out the tate of under-weight, over-weight and obese by measuring BM! thu .assessing nutrition.
Evidence shows that high BMI (obesity level) is associated with type 2 diabetes and high risk of cardiovascular morbidity and mortality.
BMI: WHO classification BM! <18.5 kg/m’ = underweight BM! 18.5 kg/m’ – 24.9 kg/m?= healthy weight range BM! 25.0 kg/m’ – 29.9 kg/m2′;’ overweight (grade I obesity) BMJ 30.0 kg/mt – 40.0 kg/m’ = obese (grade II obesity) BMI >40.0 kg/m’ = very obe e (grade III obesity)
Waist circumference
Waist circumference is measured at the level of the umbilicus. Waist circumference’ . predicts mortality better than any other anthropometric measurement. It has been proposed that waist measurement alone can be used to assess obesity, and two levels of risk have been identified.
Males Females
Level 1 > 94cm > 80 cm
Level 2 > 102 cm > 88 cm
Level 1 is the maximum acceptable waist circumference irrespective of the ‘adult age and there should be no further weight gain. Level 2 denote obesity and requires weight management to reduce the risk of type 2 diabetes and cardiovascular system complications.
Waist/llip ratio (WHR)
Waist/Hip ratio is measured as waist circumference/ hip circumference. WHR > 0.80 for women and> 0.94 for men indicate central (upper body) ‘obesity and is considered high risk for diabetes and Cardio-Vascular System (CVS) disorders. A WHR below these cut-off levels is considered low risk.
Nutritio”ul status ofpreschool (0-60 months) and other children (5-19 years)
Three nutritional indices as weight for age Z score (WAZ), height for age Z score (HAZ)., weight for height Z score (WHZ) are calculated _using World Health Organization (WHO) standard (WHO, 2006) for preschool children.
Similar indices are used along with body mass index (BMI) percentile using National Centre for Health Statistics (NCHS) (Frisancho, 1990) and also World Health Organization (WHO, 2000) for children aged 5-19 years.
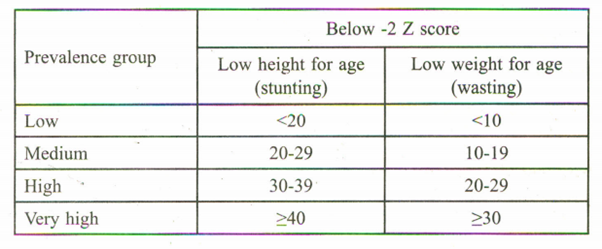
Z-score <-2 SD of the above indices are considered as underweight for WAZ, stunting for HAZ and wasting WHZ, and <51h percentile OfBMI is con idered as undernutrition. All the indices are internationally recommended (WHO, 1995).
, Worldwide classification of prevalence ranges of low height-for-age and low weightfor-age among children under 5 years of age.
Sample Questions
- 1) What do you mean by Nutrition?
- 2) Why do we consider balanced diet in maintaining good health? 3) What are recommended dietary allowances of Indians? 4) Define BM!. HoWwill you assess nutritional status through BMl in a population?